What Drives Atherosclerosis? Understanding How Heart Disease Starts and Why It Begins Early
What causes atherosclerosis? Atherosclerosis begins with the breakdown of the endothelial glycocalyx, a protective gel-like lining of the arteries. This allows ApoB-containing lipoproteins (like LDL) to penetrate the arterial wall. Once trapped, these particles trigger an immune response and chronic inflammation, leading to early plaque formation—a process that often begins as early as adolescence.
What’s in this article:
How Atherosclerosis Actually Starts: Why plaque formation is a decades-long process, not a sudden event.
Why is ApoB the Primary Driver of Risk? Understanding the difference between cholesterol weight and particle count.
The Endothelial Glycocalyx: Exploring the "inner forest" that acts as your artery's first line of defense.
ApoB vs. LDL-C: Why measuring particle number provides a more accurate picture of cardiovascular danger.
How Lp(a) Influences Genetic Risk: Identifying the inherited "risk enhancer" that standard tests often miss.
Does Heart Disease Begin in Childhood? Insights from autopsy studies on the early progression of ASCVD.
This is the first article in a 13-part series on Cardiovascular Risk & Optimization.
How Does Atherosclerosis Actually Start in the Arteries?
Atherosclerosis is the process that quietly causes most heart attacks and strokes. It doesn’t start with a dramatic event—it starts with tiny injuries inside your arteries that build over years. Understanding the root causes of atherosclerosis and early plaque formation is one of the most powerful tools you can have to protect your long-term health.
Atherosclerosis is the disease that leads to ASCVD—atherosclerotic cardiovascular disease—the umbrella term for heart attacks, strokes, and other vascular events caused by plaque buildup. When we talk about ASCVD at Ikigai, we are talking about the clinical outcomes of this long process.
Arteries are three layers thick. The innermost layer is called the intima. The intima is lined with a thin, protective layer of endothelial cells. When this lining is healthy, blood flows smoothly, inflammation stays low, and your arteries stay flexible.
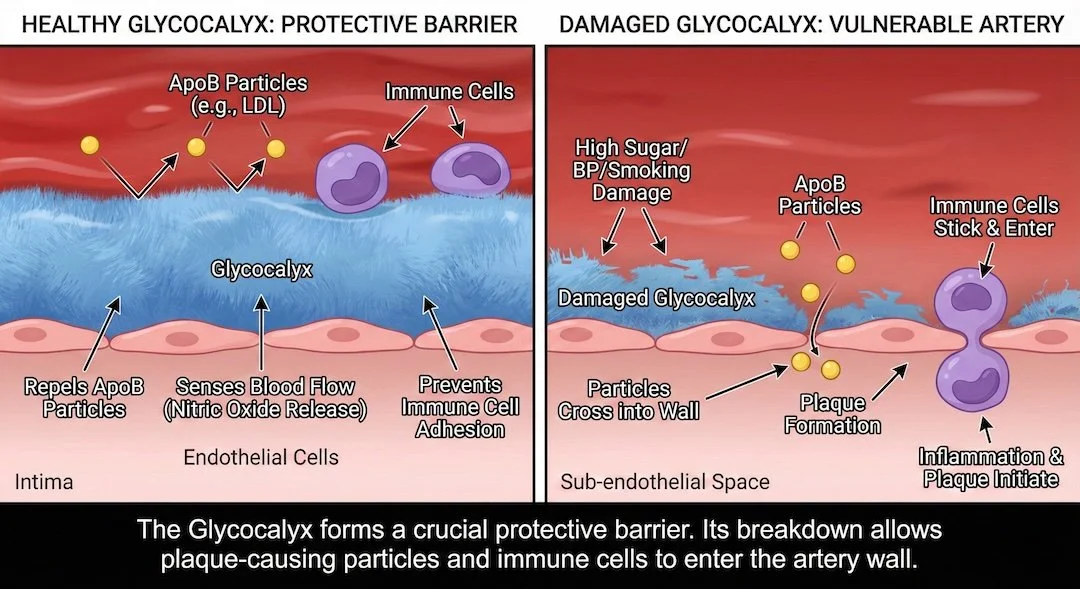
Just above these cells lies a thin, gel-like layer called the glycocalyx—the artery’s first line of defense. A healthy glycocalyx acts like a protective coating: repelling apoB-containing particles, sensing blood flow, and preventing inflammation.
Barrier protection
The glycocalyx forms both a physical and subtle electrical barrier that helps repel LDL particles and prevent them from entering the artery wall. When it is intact, it is extremely effective at keeping LDL particles out. When it thins or becomes damaged, that barrier weakens, making it far easier for these particles to cross into the endothelium and initiate atherosclerotic plaque formation.
Vascular function
The glycocalyx helps arteries sense blood flow and release nitric oxide, the molecule that keeps vessels open and flexible. Loss of glycocalyx integrity reduces nitric oxide production. This impairs the artery’s ability to dilate and promotes early atherosclerosis.
Plaque begins in the arteries when the glycocalyx breaks down.
Inflammation control
A healthy glycocalyx also helps keep inflammation in check by making it harder for immune cells to latch onto the artery wall. When the glycocalyx is worn down, those cells can stick more easily, slip underneath the surface, and begin the first steps of plaque formation.
What damages it
High blood sugar, insulin resistance, high blood pressure, smoking, oxidative stress, poor diet, and chronic inflammation accelerate glycocalyx breakdown. As the glycocalyx erodes, the endothelium becomes more vulnerable, and atherosclerosis becomes easier to initiate.
Once LDL particles cross into the artery wall, the cascade of atherosclerosis—and eventually ASCVD—begins.
Why is ApoB the Primary Driver of Cardiovascular Risk?
Why Particle Number Drives Cardiovascular Risk
Cholesterol doesn’t travel through the bloodstream on its own—it has to be carried. The particles that transport cholesterol all share a protein on their surface called apolipoprotein B, or apoB. You can think of apoB as the “license plate” that identifies each particle.
LDL particles are the most familiar, but VLDL and IDL are part of the same apoB family. Each of these particles is like a small vehicle carrying cholesterol as its passenger. What matters most for your arteries is not how much cholesterol each particle is carrying but how many of these particles are on the road at any given time—because every apoB-containing particle has the potential to enter the artery wall and contribute to plaque.

Understanding how atherosclerosis begins can help you identify your risks of heart disease, and the choices that impact your heart health.
Why Does Particle Number Matters More Than LDL Cholesterol?
Imagine moving rocks with buckets:
LDL-C tells you how full the buckets are.
ApoB tells you how many buckets you’re sending.
More buckets mean more trips into the artery wall—and more chances for plaque to form.
This is why apoB is considered a superior marker of cardiovascular risk compared to LDL cholesterol alone, and why modern guidelines recognize elevated apoB as a risk-enhancing factor.
How Does Lp(a) Increase Inherited Cardiovascular Risk?
Lipoprotein(a), or Lp(a), is an apoB-containing particle with an added apolipoprotein(a) tail that makes it more likely to stick in arteries and promote clotting. It is genetically determined, largely unaffected by lifestyle, and an important inherited risk enhancer—especially for patients with family history of premature ASCVD.
If elevated: We intensify all modifiable levers (apoB, blood pressure, inflammation, glucose) and consider advanced imaging.
Why is ApoB Necessary but Not Sufficient for Plaque Formation?
Every atherogenic lipoprotein particle contains one molecule of apoB, so apoB gives a precise count of how many risk-driving particles are in circulation.
ApoB-containing particles are necessary but not sufficient for atherosclerosis.
In the absence of elevated apoB, it is very unlikely that someone will develop ASCVD. These particles must be present—and present in excess—for plaque to form. But high apoB does not act alone. Other cardiovascular risk factors—including endothelial injury from high blood pressure, smoking, high glucose, insulin resistance, inflammation, and stress—shape how easily particles enter the artery wall and how fast disease progresses.
Elevated apoB loads the gun; other risk factors pull the trigger.
This discordance—and higher apoB at a given LDL-C—is especially common in:
diabetes
insulin resistance
metabolic syndrome
obesity
high triglycerides
While an apoB level of 130 mg/dL is considered a formal “risk-enhancing factor” by national guidelines, many large studies show rising cardiovascular risk well below this—often above ~60 mg/dL. This is why at Ikigai we look at the full picture—particle number, diet, metabolic health, blood pressure, inflammation, and imaging—to help patients keep apoB as low as safely possible for long-term protection.
Does Heart Disease Really Begin in Childhood and Adolescence?
Risk Factors You Can’t Change (But Shape Baseline Cardiovascular Risk)
These inform your baseline risk and help determine how aggressive prevention should be.
Gender
Men tend to develop ASCVD earlier.
Age
Age is one of the strongest predictors of ASCVD. Nearly everyone develops some degree of atherosclerotic plaque over a lifetime, but the amount, rate, and timing of disease vary widely from person to person. Many people develop only mild, stable plaque well into old age, while others develop high-risk plaque much earlier.
The encouraging news: while aging increases baseline risk, the burden of disease is highly modifiable. People who maintain optimal risk factors often delay ASCVD by a decade or more and experience fewer clinical events—a pattern sometimes called compression of morbidity.
How Early Atherosclerosis Starts: Evidence From Autopsy Studies
We often think of atherosclerosis as a disease of middle or older age, but decades of autopsy research show that the process begins much earlier—often in childhood and adolescence—and progresses quietly throughout young adulthood.
Studies of thousands of young people who died from trauma (not heart disease) found:
Fatty streaks—the earliest form of plaque—were nearly universal in teens and young adults.
By ages 15–19, all aortas and more than half of coronary arteries already showed early lesions.
These early changes progressed steadily from the late teens into the 30s.
Young people with more risk factors (high cholesterol, smoking, high blood pressure, obesity) had significantly more plaque, even before age 25.
Those without major risk factors had almost no advanced lesions, even into their 30s.
Atherosclerosis follows a predictable sequence: it begins in the abdominal aorta in childhood, then spreads upward to the thoracic aorta and coronary arteries over time.
What This Means for Long-Term Heart Health
Atherosclerosis is not something that suddenly appears in midlife. It is a slow, lifelong process, shaped by the biology and habits of earlier decades. Even in your 20s, 30s, and 40s, your choices—and your metabolic health—are shaping your cardiovascular future.
People who maintain healthy risk factors early in life often delay ASCVD by a decade or more, experience fewer clinical events, and compress illness into a much later part of life.
Early plaque formation is only the beginning of the story. What happens over the years—how plaques grow, change, harden, or rupture—determines whether someone eventually develops symptoms or a cardiovascular event. Protecting your endothelial glycocalyx is a fundamental strategy for maintaining cellular integrity and lowering your biological age.
In our next post—Part 2—we’ll look at how plaques behave over time and the specific steps you can take to change that trajectory.
Have questions you’d like to discuss directly? Schedule a time with us.
Recommended Reading
The Glycocalyx: The Microscopic Gatekeeper of Vascular Health – A deeper dive into the protective lining discussed in this post.
Movement as Medicine: How Exercise Protects the Heart – Learn how shear stress and nitric oxide strengthen the vascular walls against ApoB infiltration.
Understanding Lactate: Your Real-Time Metabolic Health Biomarker – Why mitochondrial efficiency is key to preventing the metabolic "triggers" of heart disease.
Executive Vitality: Why Your Physiology is Your Best Business Strategy – How the Ikigai process identifies hidden cardiovascular risks in high-performers.